Dein AAPS-Profil
Dein AAPS-Profil hat fünf wichtige Parametern, die definieren, wie AAPS Insulin als Reaktion auf Deine Sensorglukosewerte abgeben soll. Dies sind die Hauptparameter auf denen AAPS aufbaut. Während Du Dich durch die Ziele arbeitest, wirst Du weitere einstellbare Parameter (wie SMB-Einstellungen) freischalten. Die Wirksamkeit dieser Funktionen hängt aber hauptsächlich davon ab, dass Dein zugrundeliegendes Profil korrekt ist. Das Profil enthält:
Insulinwirkdauer (DIA; engl. duration of insulin action),
Basalraten (BR),
Insulinempfindlichkeits- / Korrekturfaktoren (ISF; engl. insulin sensitivity factors) und
Mahlzeitenfaktoren / KH-Faktoren (IC oder ICR; engl. insulin-to-carb ratios).
Im Rahmen des AAPS-Managements sollten Nutzende ihre Profil--Einstellungen kontinuierlich auf ihre Passgenauigkeit anschauen und bewerten. Es wird empfohlen, die Einstellungen in der Reihenfolge vorzunehmen, wie es hier dargestellt ist. Stelle sicher, dass die Einstellung wirklich richtig ist, bevor Du die jeweils nächste in Angriff nimmst. Taste dich in kleinen Schritten voran, statt zu viele Änderungen auf einmal vorzunehmen. Vergiss nicht nach jeder Änderung Dein Profil auch zu aktivieren. Sichere Deine Profil-Einstellungen regelmäßig, in dem Du die Einstellungen exportierst.
Deine Profil-Einstellungen hängen voneinander ab - Du kannst u. U. „schiefe“ Einstellungen haben, die in bestimmten Situationen gut zueinander passen, aber in anderen Situationen überhaupt nicht funktionieren. Wenn zum Beispiel ein zu hohes Basal auf einen zu hohen (schwachen) CR (Mahlzeit-Faktor) trifft. Das bedeutet, dass Du die Einstellungen individuell betrachten und überprüfen musst, ob sie unter den verschiedenen Bedingungen gut funktionieren.
Du kannst Autotune zwar als Ausgangspunkt für Deine Überlegungen verwenden, solltest ihm aber nicht blind vertrauen: Es funktioniert unter Berücksichtigung aller individuellen Einflüsse möglicherweise bei Dir nicht gut genug.
Your diabetes may vary
Profile unterscheiden sich von Person zu Person sehr.
Für die restlichen drei Parameter Basalrate (BR), Insulinempfindlichkeitsfaktoren (ISF) und Insulin-Kohlenhydrat-Verhätnisse bzw. Mahlzeitenfaktoren (IC oder ICR), variieren die absoluten Werte und Trends Deines Insulinbedarfs. Der Insulinbedarf ist dabei abhängig von Deiner Biologie, Geschlecht, Alter, Fitnessgrad usw., aber auch von vorübergehenden Einflüssen wie Krankheit und sportlicher Aktivitität und variiert mitunter erheblich. Für tiefere Einblicke in das Thema wird das englischsprachige Buch “Brights Spots and Landmines” von Adam Brown empfohlen.
Die vier letzten Parameter (Glukoseziele, Basalraten, Insulinempfindlichkeitsfaktoren und Mahlzeitfaktoren) können auf unterschiedliche Werte eingestellt werden, die bei Bedarf stündlich wechseln.
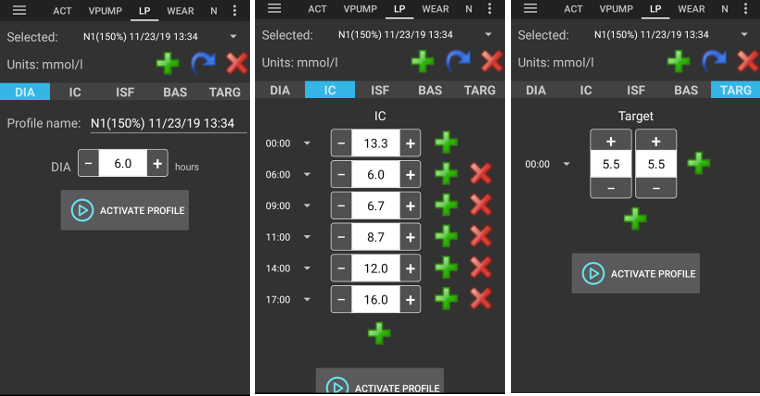
AAPS-Screenshots eines Beispiel-Profils sind unten zu sehen. Dieses Beispielprofil enthält sehr viele Zeitfenster. Wenn Du mit AAPS startest, hast Du wahrscheinlich ein deutlich einfacheres Profil.
Insulinwirkdauer (DIA)
Beschreibung
Die Zeit, die das Insulin braucht, bis es keine Wirkung mehr zeigt.
Da Deine Pumpe nur ein Insulinart abgibt, ist die Insulinwirkdauer in AAPS auch nur durch einen Wert festgelegt.
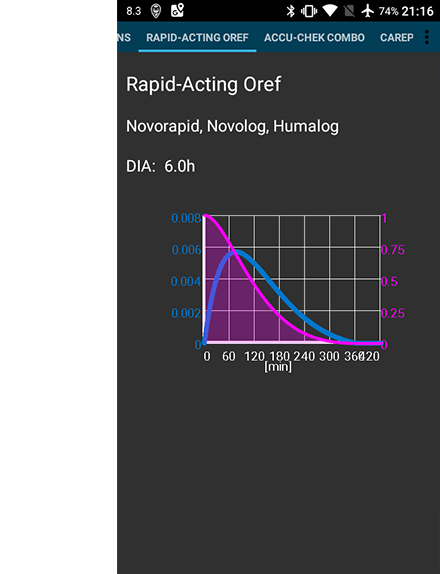
In Kombination mit dem Insulintyp führt das zu einem Insulinprofil, wie es im obigen Bild dargestellt ist. Wichtig zu beachten ist, dass der Abbau, d.h. die Wirkung deutlich länger anhält (sog. „long tail“), als gemein hin angenommen wird. Wenn Du Deine Pumpe bisher manuell eingesetzt hast, bist Du wahrscheinlich von wesentlich kürzeren Insulinwirkdauern (etwa 3,5 Stunden) ausgegangen. Allerdings spielt der langsamere Abbau beim Loopen eine wichtige Rolle, da die Berechnungen deutlich präziser sind und sich diese geringen Mengen unter den rekursiven Berechnungen des AAPS-Algorithmus aufsummieren. AAPS verwendet daher einen DIA-Wert von mindestens 5 Stunden.
Ausführlichere Lektüren zum Thema Insulinwirkdauer und warum diese relevant ist:
Understanding the New IOB Curves Based on Exponential Activity Curves in der OpenAPS-Dokumentation.
Why we are regularly wrong in the duration of insulin action (DIA) times we use, and why it matters… auf Diabettech.
Exponential Insulin Curves + Fiasp auf See My CGM (Archiv).
Revised Humalog model in a closed loop und weitere Artikel auf Bionic Wookie, empfehlen einen DIA-Wert von 9 Stunden für Lyumjev, Fiasp, Novorapid, Humalog.
Auswirkung
Ein zu kurze Insulinwirkdauer (DIA) kann zu niedrigen Glukosewerten führen. Und umgekehrt.
Wenn die Insulinwirkdauer (DIA) zu kurz ist, errechnet AAPS, dass das Restinsulin zu früh verbraucht ist und gibt im Falle eines hohen Glukosewerts dann zu viel Insulin ab. (Tatsächlich wartet AAPS nicht die volle Insulinwirkdauer ab, sondern sagt die Entwicklung der Glukosewerte vorher und gibt entsprechend Insulin ab oder nicht). Dies führt im Wesentlichen zu einem „Insulin-Stau“ (engl. Insulin-Stacking), von dem AAPS nichts weiß. Das ist besonders Nachts sichtbar, wenn Du negatives IOB erkennst, für das alle anderen Erklärungen, außer einer noch anhaltenden Wirkung des letzten Bolus, ausscheiden.
Ein Beispiel für einen zu kurzen DIA ist ein hoher Glukosewert, der durch die AAPS-Überkorrektur in einem niedrigen Glukosewert endet.
Wie es eingestellt wird
Die Abbildung unten zeigt ein Beispiel einer im AAPS-Profil gesetzten Insulinwirkdauer (DIA).

Der DIA-Wert wird zu Beginn häufig zu klein gewählt. Eine DIA mit 6 oder 7 ist wahrscheinlich ein guter Ausgangspunkt. Für immer mehr Menschen scheint ein DIA von 8 bis 9 Stunden gut zu funktionieren. Schau Dir hierzu die oben erwähnte weiterführende Lektüre an.
Glukoseziele
Beschreibung
Dein Glukoseziel ist der zentrale Wert. Alle AAPS-Berechnungen basieren darauf. Er ist nicht der Zielbereich, in dem Du normalerweise versuchst Deine Glukosewerte zu halten. Das Glukoseziel wird in AAPS-Berechnungen verwendet: Wenn AAPS voraussagt, dass Dein Glukosewert außerhalb des Zielbereichs landen wird, wird es Maßnahmen ergreifen, um wieder in den Bereich zurückzukommen.
The targets can be defined within those boundaries :
Unteres Ziel |
Oberes Ziel |
|
|---|---|---|
Minimum |
4 mmol/l oder 72 mg/dl |
5 mmol/l or 90 mg/dL |
Maximum |
10 mmol/l or 180 mg/dL |
15 mmol/l oder 225 mg/dl |
Auswirkung
Wenn das Glukoseziel in Deinem Profil sehr breit ist (sagen wir, 3 oder mehr mmol/l [50 mg/dl oder mehr), wird AAPS selten eingreifen. Das liegt daran, dass der vorhergesagte Glukosewert innerhalb des weiten Bereichs befindet und es daher unwahrscheinlich ist, dass AAPS mit Änderungen der temporären Basalrate reagieren wird.
Wie es eingestellt wird
Die Abbildung unten zeigt ein Beispiel wie im AAPS-Profil das Glukoseziel hinterlegt werden kann.

Glukoseziele werden so gesetzt, dass sie zu Deinen eigenen Wünschen und Anforderungen passen. Wenn Du beispielsweise Angst vor nächtlichen Hypos hast, kannst Du Dein Glukoseziel von 21.00 - 07.00 Uhr auf 117 mg/dl setzen (6,5 mmol/l) setzen. Wenn Du erreichen möchtest, dass Du vor dem Frühstücksbolus am Morgen bereits genügend aktives Insulin (IOB) im Körper hast, könntest Du für die Zeit von 07.00 - 08.00 Uhr ein niedrigeres Ziel von 81 mg/dl (4,5 mmol/dl) setzen.
Wenn Du im Open Loop und insbesondere beim Durchlaufen der ersten Ziele bist, gerade lernst wie sich AAPS verhält und/oder Du Dein Profil anpasst, kann es helfen den Zielbereich etwas weiter zu wählen.
Sobald Du in den Closed Loop (beginnend mit dem Ziel 6) wechselst, wird empfohlen den Zielbereich für jeden Tagsabschnitt bis auf einen einzelnen Zielwert (unteres Ziel = oberes Ziel) zu verkleinern. Damit kann AAPS schnell auf Glukosewert-Schwankungen reagieren.
Basalraten
Beschreibung
Deine Basalrate ist die Insulinmenge (Einheiten pro Stunde), die abgegeben wird, um Deinen Glukosewert ohne Nahrung und Sport stabil zu halten
Die Insulinpumpe liefert alle paar Minuten kleine Mengen schnell wirkendes Insulins, um die durch die Leber abgegebene Glukose entsprechend in die Körperzellen zu bringen. Basalinsulin macht typischerweise 40 - 50% Deines täglichen Gesamtinsulinbedarfs (TDD) aus und ist abhängig von Deinen Ernährungsgewohnheiten. Es folgt üblicherweise Deinem Biorhythmus (cirkadianes Muster) mit einer Spitze und einem Tal im täglichen Insulinbedarf. Für weitere Informationen ist das Kapitel 6 des englischsprachigen Buches “Think like a Pancreas” von Gary Scheiner lesenswert.
Die meisten Diabetes-Teams (und Menschen mit Typ-1-Diabetes!), stimmen darin überein, dass Basalraten vor ISF und ICR optimiert werden sollten.
Auswirkung
Saubere Basalraten ermöglichen Dir Morgens mit Werten im Zielbereich wachzuwerden, Mahlzeiten auszulassen, früher oder später essen zu können ohne hohe oder niedrige Werte zu bekommen.
Eine zu hohe Basalrate kann zu niedrigen Glukosewerten führen. Und umgekehrt.
Die Standard-Basalrate ist der Referenzwert für AAPS. Wenn die Basalrate zu hoch ist, führt ein ‚zero temp‘ (temporäres Abschalten der Basalrate durch AAPS) zu einem höheren negativen IOB (insulin on board - im Körper aktives Insulin) als es sollte. Dies wird dazu führen, dass AAPS häufiger korrigiert als es tatsächlich notwendig wäre, um am Ende IOB auf Null zu bringen.
Eine zu hohe Basalrate führt also zu niedrigen Glukosewerten sowohl durch die Standard-Basalrate als auch später durch die Korrekturen von AAPS auf den Zielwert.
Umgekehrt kann eine zu niedrige Basalrate zu zu hohen Glukosewerten führen und AAPS daran hindern, diese wieder in den Zielbereich zu bringen.
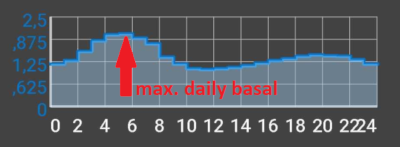
Wie es eingestellt wird
Die Abbildung unten zeigt ein Beispiel, wie im AAPS-Profil die Basalrate hinterlegt werden kann.

Die richtige Basalrate zu finden ist ein „Trial and Error“-Prozess, und sollte in Abstimmung mit Deinem Diabetes-Team erfolgen.
Basalraten-Tests bringen es normalerweise mit sich, während einer begrenzten Fastenperiode in einem 24-Stunden Zeitraum die Basalrate und den Insulinbedarf zu beobachten. Auch wenn die Basalrate für einen ganzen Tag getestet werden muss, ist es nicht empfehlenswert 24 Stunden am Stück zu fasten. Das liegt daran, dass der Körper über spezielle Mechanismen versuchen wird das Fasten (z. B. durch Hormonausschüttung) auszugleichen. Eine empfohlene Methode ist 3 Mal für einen Zeitraum von 8 Stunden zu fasten.
Das empfohlene Vorgehen ist, den Loop zu deaktivieren (als Vorsichtsmaßnahme kann AAPS - wie Du es schon zum Erreichen des Ziel 6 gemacht hast - in den Modus LGS gebracht werden). So kannst Du niedrige Werte vermeiden und es wird später automatisch auf die hinterlegte Standard-Basalrate zurückgekehrt. Beobachte wie sich Dein Glukosewert entwickelt: Sinkt er, ist die Basalrate zu hoch. Und umgekehrt.
Eine andere (möglicherweise schwierigere) Methode ist, den Loop aktiv zu lassen und zu beobachten, wie sich das IOB verändert. Wenn das IOB negativ ist, ist Deine Basalrate zu hoch. Und umgekehrt. Beachte, dass diese Methode den ISF nutzt, um damit den Glukosewert zu korrigieren. Damit hängt der Erfolg von mehreren Variablen (und nicht nur von der Basalrate) ab.
Eine weitere Möglichkeit die Basalrate anzuzupassen ist, die Loop-Aktionen während der Nacht, wenn keine Kohlenhydrate mehr aktiv sind, zu beobachten. Diese Methode ist besonders für Kinder, für die Fasten oft schwierig ist oder deren Insulinbedarf sich oft ändert, geeignet. Dr. Saleh Adi von Tidepool bietet hilfreiche Wege, wie Du nächtliche Glukoseverläufe analysieren kannst und daraus Optimierungen der Basalrate ableiten kannst, an.
Hier erfährst Du durch das Analysieren von Mustern im Closed Loop, wie Du Dein Basalprofil feinjustieren kannst.
Wenn Du auf Basis der Ergebnisse des Basalratentests Veränderungen vornehmen möchtest, sollten diese im Profil 1 bis 2 Stunden (abhängig vom Insulintyp) vor dem Anfstieg/Abfall eingearbeitet werden. Wiederhole den Test so lange, bis Du mit Deiner Basalraten-Einstellungen zufrieden bist.
Insulinempfindlichkeitsfaktor („Korrekturfaktor“)
Beschreibung
Der Insulinempfindlichkeitsfaktor (manchmal auch Korrekturfaktor genannt) ist ein Maß dafür, wie viel der Glukosewert durch eine Insulineinheit gesenkt wird.
In mg/dl-Einheiten: Wenn Dein ISF 40 ist, senkt jede Insulineinheit Deinen Glukosewert um ca. 40 mg/dl (z. B. von 140 mg/dl auf 100 mg/dl).
In mmol/l-Einheiten: Wenn Dein ISF 1,5 ist, senkt jede Insulineinheit Deinen Glukosewert um 1,5 mmol/l (z. B. von 8 mmol/l auf 6,5 mmol/l).
An diesen Beispielen kannst Du erkennen, dass kleinerer ISF-Werte geringere Insulinempfindlichkeit bedeutet. Wenn Du also Deinen ISF von 40 auf 35 (mg/dl) oder 1,5 auf 1,3 (mmol/l) senkst, wird dies oft als verstärken des ISF bezeichnet. Umgekehrt schwächt die Erhöhung des ISF-Wertes von 40 auf 45 (mg/dl) oder von 1,5 auf 1,8 mmol/l) Deinen ISF.
Auswirkung
Eine niedrigerer / stärkerer ISF (z. B. 40 statt 50) bedeutet, dass das Insulin Deinen Glukosewert mit einer Einheit weniger stark senkt. Dies führt dazu, dass der Loop mit mehr Insulin aggressiver / stärker korrigiert. Ist Dein ISF zu stark (kleiner Wert), kann das zu niedrigen Glukosewerten führen.
Ein höherer / schwächerer ISF (z. B. 45 statt 35) bedeutet, dass das Insulin Deinen Glukosewert mit einer Einheit stärker senkt. Dies führt zu einer weniger aggressiven / schwächeren Korrektur des Loops mit weniger Insulin. Ist Dein ISF zu schwach (großer Wert), kann dies zu hohen Glukosewerten führen.
Beispiel:
Der Glukosewert ist 190 mg/dl (10,5 mmol/l) und das Ziel ist 100 mg/dl (5,6 mmol/l).
Du möchtest also eine Korrektur um
190 - 110 = 90 mg/dloder10,5 - 5,6 = 4,9 mmol/lWenn
ISF = 30->90 / 30 = 3oderISF = 1,3->4,9 / 1,63 = 3: 3 Einheiten InsulinWenn
ISF = 45->90 / 45 = 2oderISF = 2,45->4,9 / 2,45 = 2: 2 Einheiten Insulin
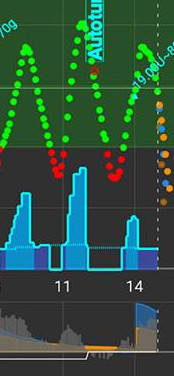
Ein zu niedriger ISF (und daher zu aggressiver; nicht unüblich) kann zu „Überkorrekturen“ führen. AAPS errechnet, dass mehr Insulin benötigt wird, um einen hohen Glukosewert zu korrigieren. Dies kann (besonders während des Fastens) zu einem „Achterbahn“-Verlauf der Glukosewerte führen, so wie es auf dem Bild unten dargestellt ist. In diesen Situationen sollte der ISF-Wert erhöht werden, um AAPS so weniger aggressiv zu machen. Dadurch wird sichergestellt, dass AAPS kleinere Korrekturdosen abgibt, und vermeidet damit die Überkorrektur eines hohen Glukosewertes, die einen niedrigen Glukosewert zur Folge haben würde.
Umgekehrt kann ein zu hoher ISF zu zu schwachen Korrekturen führen. Dies bedeutet, dass Deine Glukosewerte - besonders in der Nacht - oberhalb Deines Zielwertes bleiben.
Wie es eingestellt wird
Die Abbildung unten zeigt an einem Beispiel, wie ISF-Werte in einem AAPS-Profil eingetragen werden können.

Eine Möglichkeit einen ersten Wert für den ISF am Tage zu ermitteln, nutzt Deinen tägliches Gesamtinsulinbedarf (TDD) und die 1700- bzw. 94-Regel. Für weitere Informationen ist das Kapitel 7 des englischsprachigen Buches “Think like a Pancreas” von Gary Scheiner lesenswert.
1700 (beim Messen in mg/dl) oder 94 (mmol/l)/ TDD = ca. |
|---|
Wenn Du der Meinung bist, dass Deine Basalrate passt, kannst Du sie testen, indem Du den Loop pausierst, sicherstellst, dass das IOB Null ist, und Du Deinen Glukosewert z. B. mit Traubenzucker auf ein hohes und stabiles Niveau bringst.
Gebe dann die Deinem Korrekturfaktor entsprechende Menge Insulin ab, um wieder zu Deinem Zielwert zu gelangen.
Sei vorsichtig, da die Korrektur oftmals zu aggressiv eingestellt ist. D.h. eine Einheit Insulin senkt den BZ stärker als Du denkst.
Insulin-Kohlenhydrat-Verhältnis (insulin to carb ratio - ICR)
Beschreibung
Der ICR ist ein Maß dafür, wie viele Gramm Kohlenhydrate von einer Insulineinheit abgedeckt werden. Ergänzung: Im Deutschen werden diese manchmal auch Mahlzeitenfaktoren genannt.
Teilweise wird auch I:C statt ICR als Abkürzung verwendet oder vom Kohlenhydratverhältnis (carb ratio - CR) gesprochen.
Zum Beispiel bedeutet ein Insulin-Kohlenhydrat-Verhältnis von 1 zu 10 (1:10), dass Du eine Einheit Insulin pro 10g Kohlenhydrate benötigst. Ein Essen mit 25 g Kohlenhydraten würde 2,5 Einheiten Insulin benötigen.
Wenn Du einen schwächeren ICR-Wert (hoher Wert) hast, z. B. 1:20, würdest Du nur 0,5 IE Insulin zum Abdecken von 10 g Kohlenhydraten benötigen. Ein Essen mit 25g Kohlenhydraten würde 25/20 = 1,25 IE Insulin benötigen.
Aufgrund von Hormonen und sportlichen Aktivitäten ist es normal, über den Tag verteilt unterschiedliche ICR-Werte zu haben. Viele Menschen haben rund um die Frühstückszeit ihren niedrigsten/stärksten ICR, da es dort potenziell stärkere Insulinresistenzen gibt. So könnte für einen Erwachsenen zum Beispiel der ICR-Wert 1:8 zum Frühstück, 1:10 zum Mittagessen und 1:10 zum Abendessen sein. Doch dieses Muster lässt sich nicht verallgemeinern. Einige Menschen sind zum Abendessen insulinresistenter und benötigen dann ein stärkeres/kleineres ICR.
HINWEIS:
In manchen Europäischen Ländern wurden sog. Broteinheiten (BE) genutzt um festzulegen, wie viel Insulin für Lebensmittel benötigt wird. Zu Beginn entsprach eine BE 12g Kohlenhydraten, später haben manche dies auf 10g Kohlenhydrate geändert.
Bei diesem Modell war die Menge der Kohlenhydrate fix während die Insulinmenge variierte. („Wie viel Insulin benötige ich für eine BE?“)
Beim ICR hingegen ist die Insulinmenge fix und die Menge der Kohlenhydrate variiert. („Wie viele Gramm Kohlenhydrate können mit einer Einheit Insulin abgedeckt werden?“)
Beispiel:
BE-Faktor (BE = 12g KH): 2,4 IE/BE -> Du benötigst 2,4 Einheiten Insulin, wenn Du eine BE isst.
Dazu passender ICR: 12 g / 2,4 IE = 5,0 g/IE -> Du kannst 5,0 g Kohlenhydrate essen, wenn Du sie mit einer Einheit Insulin abdeckst.
BE-Faktor 2,4 IE / 12 g ===> IC = 12 g / 2,4 IE = 5,0 g/IE
Umrechnungstabellen finden sich online z.B. hier.
Auswirkung
Eine niedrigeres / stärkeres ICR bedeutet weniger Nahrung pro Einheit, d.h. Du erhältst mehr Insulin für eine feste Kohlenhydratmenge. Man kann dies auch als „aggressiver“ bezeichnen. Wenn der IC-Wert zu stark ist, bekommst Du zu viel, was niedrige Glukosewerte nach sich ziehen kann.
Ein höheres / schwächeres ICR = mehr Kohlenhydrate pro Insulineinheit, d.h. Du bekommst für eine gleichbleibende Kohlenhydratmenge weniger Insulin. Man kann dies auch als „schwächer“ oder „weniger aggressiv“ bezeichnen. Wenn Dein IC-Wert zu schwach ist, bekommst Du weniger Insulin als Du tatsächlich brauchst. Das kann hohe Glokusewerte zur Folge haben.
Wie es eingestellt wird
Die Abbildung unten zeigt beispielhaft das ICR einer Person und wie es in einem AAPS-Profil eingetragen werden kann. Bei der Eingabe dieser Werte geben wir einfach den letzten Teil des Verhältnisses ein, sodass ein Insulin-zu-Koherlnhudrat-Verhältnis von 1:3,5 als „3,5“ eingegeben wird.

Wenn ein Essen verdaut wurde und das IOB auf Null zurückgekehrt ist, Dein Glukosewert aber höher als vor dem Essen bleibt, ist es wahrscheinlich, dass Dein ICR zu schwach ist (_d. h. _ der Wert ist zu hoch und sollte schrittweise gesenkt werden). Im umgekehrten Fall, der Glukosewert ist niedriger als vor der Mahlzeit, ist das ICR ist zu stark (d. h. der Wert ist zu klein und sollte schrittweise erhöht werden).
Wenn Du annimmst, dass Deine Basalrate stimmt, Dein IOB Null ist und Du im Zielbereich bist, dann kannst Du - basierend auf Deinen aktuellen Einstellungen - den ICR-Wert testen. Iss eine genau bekannte Kohlenhydratmenge und gib die Insulinmenge ab, die sich aus Deinem aktuellen Mahlzeitfaktor (ICR) ergibt. Am besten isst Du Nahrungsmittel, die Du zu dieser Tageszeit üblicherweise isst und bestimmst deren Kohlenhydratmenge präzise.
Häufige zum Profil auftretende Fragen
About the importance of getting your profile right
Warum sollte ich versuchen, meine Profileinstellungen richtig zu haben? Kann sich der Loop nicht darum kümmern?
Ein Hybrid Closed Loop kann versuchen, die Insulinzufuhr anzupassen, um eine schlechte glykämische Kontrolle, die die Folge aus falschen Profilwerten ist, zu verbessern. It can do this, for example, by withholding insulin delivery if you are going to hypo. Du kannst eine deutlich bessere glykämische Kontrolle erreichen, wenn Deine Profilwerte so nah wie möglich am Bedarf Deines Körpers sind. Dies ist einer der Gründe, warum AAPS abgestufte Ziele für den Übergang vom Open Loop zum Hybrid Closed Loop setzt. Zusätzlich gibt es Situationen (Sensor-Aufwärmphase, Sensorfehler etc.), in denen der Loop geöffnet bzw. unterbrochen werden muss. Manchmal passiert das mitten in der Nacht und Du wirst dann für die richtigen Einstellungen dankbar sein.
Wenn Du von einem anderen Open oder Closed Loop Pumpensystem auf AAPS umsteigst, hast Du vermutlich schon eine recht gute Vorstellung von Deiner Basalrate (BR), Deinen Insulinempfindlichkeitsfaktoren (ISF) und Deinen Insulin-Kohlenhydrat-Faktoren bzw. Mahlzeitenfaktoren (ICR).
Wenn Du von der Pen-Therapie (z. B. ICT) zu AAPS wechselst, solltest Du Dich zunächst mit dem Umstieg vom Pen auf die Insulinpumpe beschäftigen, bevor Du den wohlüberlegten Wechsel gemeinsam mit Deinem Diabetes-Team angehst. „Pumping insulin“ von John Walsh & Ruth Roberts und „Think like a Pancreas“ von Gary Scheiner sind sehr lesenswert.
Was sind die Ursachen hoher postprandialer Peaks im Closed Loop?
Zuerst solltest du deine Basalrate prüfen und einen Basalratentest ohne Kohlenhydrate machen. Wenn Deine Basalrate korrekt ist und Dein Glukosewert nach voller KH-Absorption auch wieder bis zu Deinem Zielwert fällt, versuche einmal das temporäre Ziel „Bald Essen“ in AAPS einige Zeit vor der Mahlzeit zu setzen oder überlege zusammen mit Deinem Diabetologen oder Deiner Diabetologin, welcher Spritz-Ess-Abstand (SEA) geeignet wäre.
Wenn Dein Glukosewert nach dem Essen zu hoch ist und nach der vollständigen Verstoffwechselung der Kohlenhydrate immer noch zu hoch ist, denke gemeinsam mit Deinem Diabetes-Team über einen kleineren / stärkeren ICR-Wert nach. Wenn bei aktiven Kohlenhydraten (COB) Deine Glukosewerte zu hoch und nach der vollständigen Verstoffwechselung zu niedrig sind, denke gemeinsam mit Deinem Diabetes-Team über einen größeren / schwächeren ICR-Wert und einen geeigneten SEA nach.
Ich stecke in hohen Werten fest und der Loop bringt mich nicht herunter
Die möglichen Gründe dafür, dass AAPS nicht genug Insulin abgibt, sind:
ISF ist nicht stark genug
Das Basal könnte zu schwach sein
Eine Sicherheitseinstellung (z. B. maxIOB) kann ausgelöst haben. Oder SMB sind zu diesem Zeitpunkt ausgeschaltet. Das ist von Deinen Einstellungen abhängig.
Eine Automatisierung ist aktiv und hat die AAPS-Entscheidung überschrieben.
Ich habe negatives IOB, ist das ein Problem?
Negatives IOB bedeutet, dass die Gesamtmenge des in Deinem Körper aktiven Insulins (Basal + Bolus) kleiner ist als das Basal. Das wird dazu führen, dass AAPS, sobald die Glukosewerte steigen mehr Insulin abgeben wird, um das vorher zurückgehaltene Insulin „aufzuholen“. Das kann in der Folge dann zu niedrigen Glukosewerten führen.
Hier jetzt einige Gründe für das Entstehen negativen IOBs und mögliche Reaktionen darauf:
Ein zu starkes Basal: Optimiere Dein Profil
Ein zu großer Mahlzeiten-Bolus: Optimiere Dein Profil oder überprüfe, ob Du zum richtigen Zeitpunkt bolst.
DIA ist zu kurz und führt zu „Insulin Stacking“: Passe Dein Profil an
Bewegung: Beim nächsten Mal solltest Du während (eventuell bereits vor) der Aktivität ein reduziertes prozentuales Profil nutzen, um so der höheren Insulin-Empfindlichkeit gerecht zu werden.
Deine Profile verwalten
Profile erstellen und bearbeiten
Der Profil-Reiter ist, abhängig von Deinen Einstellungen in der Konfiguration, entweder im oberen Menü oder im Hamburger Menü, zu finden.
Schaltflächen:
grünes Plus: hinzufügen
rotes X: löschen
blauer Pfeil: duplizieren
Bei Änderungen an Deinem Profil, achte darauf, dass Du sie an dem richtigen Profil vornimmst. Beim Wechsel zum Profil-Tab wird nicht immer das aktuell genutzte Profil angezeigt. Wenn Du z. B. einen Profilwechsel über den Startbildschirm durchgeführt hast, wird ggf. im Profil-Tab ein anderes Profil angezeigt.
Ein völlig neues Profil für ein Kind erstellen
Der Profil-Helfer -Tab kann Dir beim Erstellen eines Profils für Kinder bis 18 Jahren helfen.
Wichtiger Hinweis:
Profil-Helfer soll Dich dabei unterstützen, das anfängliche Profil für Dein Kind zu finden. Auch wenn es auf Datensätzen von zwei verschiedenen Krankenhäusern basiert, besprich es immer mit Deinem medizinischen Team, bevor Du ein neues Profil benutzt!
Profil-Helfer bietet Datensätze von zwei verschiedenen Kinderkrankenhäusern an, um ein anfängliches Profil für Dein Kind (bis 18 Jahre) zu finden.
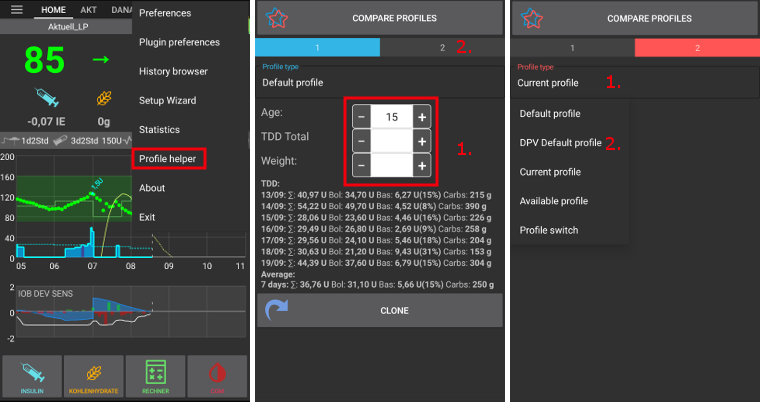
Achte darauf, dass Du im Profil 1 bist.
Als Profil-Typ, wählst Du „Standard-Profil“ aus.
Passe das Standardprofil (basierend auf dem Krankenhausdatensatz) an, indem Du das Alter des Kindes eingibst sowie entweder das Gesamt-TDD oder das Gewicht eingibst.
Wechsle durch das Tippen auf Profil 2 oben rechts auf den anderen Bildschirm.
Tippe auf Profil-Typ und wähle das „DPV-Standard-Profil“ aus.
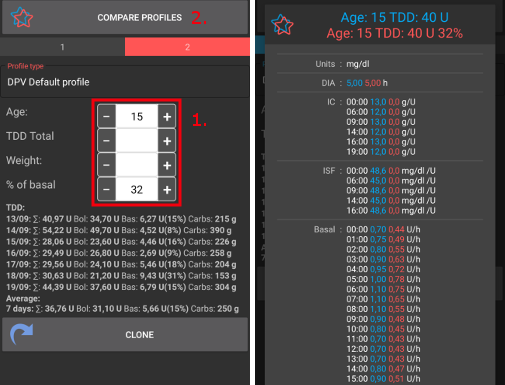
Passe das DPV-Standardprofil (basierend auf einem anderen Krankenhausdatensatz) an, indem Du das Alter des Kindes, den Prozentsatz der Basalrate sowie entweder das Gesamt-TDD oder das Gewicht eingibst.
Tippe unten auf dem Bildschirm auf Profile vergleichen. Ein Vergleich der beiden angepassten Profile wird angezeigt (siehe Screenshot unten).
Um Dein Profil auf Basis einer dieser Vorschläge zu optimieren, tippe auf den Klonen-Button des Profil 1 oder Profil 2.
Profil wechseln
Mehr Informationen findest Du im Abschnitt Profilwechsel & Prozentuale Profilanpassung.
Einen Profilwechsel in ein neues Profil klonen

Auf dem Reiter Behandlungen werden alle durchgeführten Profilwechsel angezeigt. Wenn Du auf den Sub-Reiter Profilwechsel gehst, kannst Du dort einen bereits erfolgten Profilwechsel als Basis für ein neues Profil nutzen. Zeitverschiebung und Prozentsatz des Profilwechsels werden in das lokale neue Profil übernommen. Tippe auf Klonen in Zeile 1.
Du kannst jetzt auf den Profil-Reiter wechseln und dort das neu erstelle Profil bearbeiten.
Sicherung Deines Profils
Die Profile sind die wichtigste Einstellung Deines Loop-Systems. Die Profile sind höchst empfindlich und etwas, was Du auf keinen Fall verlieren möchtest.
Deine Profile werden in der AAPS-Datenbank gespeichert.
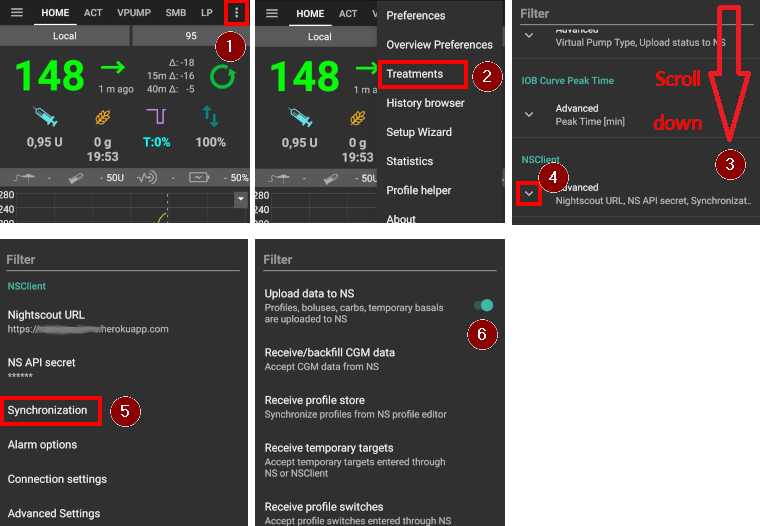
Falls aktiviert, werden Profile auch zu Nightscout hochgeladen. Die Einstellungen findest Du unter Einstellungen > Nightscout-Client > Synchronisierung > Daten zu NS hochladen.
Sie sind auch in den exportierten Einstellungen enthalten. Stelle also sicher, dass Du immer ein Backup an einem sicheren Ort hast.
Profile über Nightscout bearbeiten
Wenn aktiviert, kommen Profiländerungen, die direkt in Nightscout vorgenommen wurden, auch in AAPS an. Die Einstellungen findest Du unter Einstellungen > Nightscout-Client > Synchronisierung > Gespeicherte Profile abrufen.
Wenn Du gravierende Änderungen an einem umfangreichen Profil vorgenommen hast, kann diese Funktion hilfreich sein. Es ist in der Regel deutlich einfacher diese Änderungen, z.B. Daten aus einem Arbeitsblatt zu kopieren, über das Web-Interface zu machen.
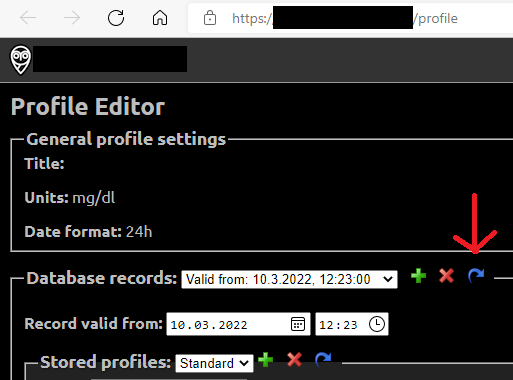
Es ist dabei wichtig, den gesamten -Datenbank-Datensatz, der aus mehreren Profilen im Nightscout-Editor besteht (blauer Pfeil auf dem Screenshot unten), zu klonen. Der neue Datensatz enthält dann das aktuelle Datum. Nach dem Speichern kann das geänderte/neue Profil in AAPS mit einem regulären Profilwechsel aktiviert werden.
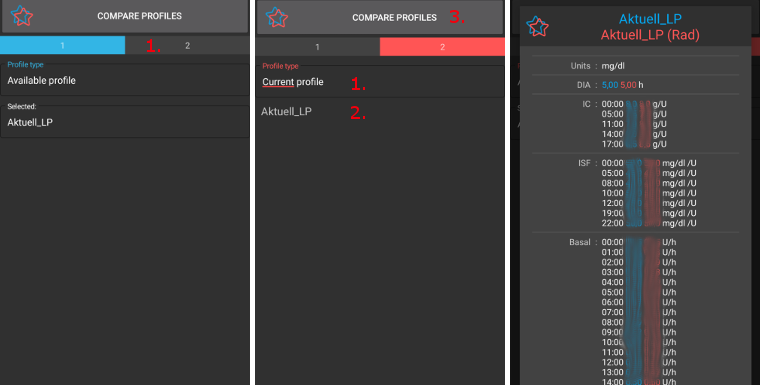
Vergleiche zwei Profile
Du kannst den Profil-Helfer auch verwenden, um Profile oder Profilwechsel (um einen Prozentsatz geändertes Profil) miteinander zu vergleichen.
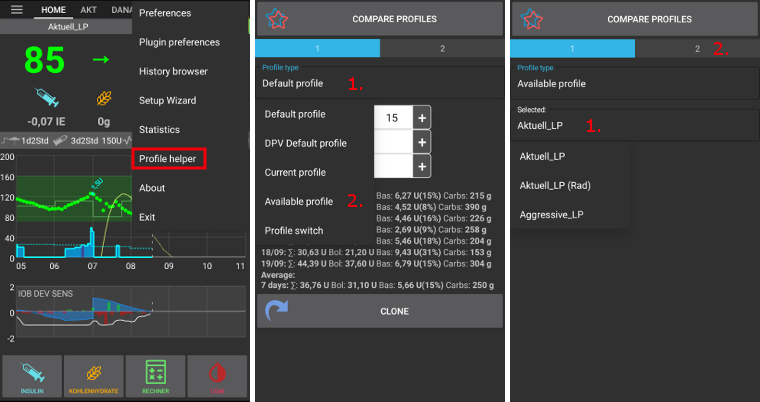
Achte darauf, dass Du im Profil 1 bist.
Wähle im Profil-Typ „Verfügbares Profil“ aus und wähle aus allen gespeicherten Profilen aus.
Wähle das Profil aus, gegen das Du vergleichen möchtest.
Wechsle durch das Tippen auf Profil 2 oben rechts auf den anderen Bildschirm.
Wähle im Profil-Typ „Profilwechsel“ aus, um im Verlauf aus allen erfolgten Profilwechseln auszuwählen.
Wähle das Profilwechsel aus, gegen den Du vergleichen möchtest.
Tippe unten auf dem Bildschirm auf Profile vergleichen. Ein Vergleich der beiden angepassten Profile wird angezeigt (siehe Screenshot unten).